
INFANT HIP ULTRASOUND
Why take a child for hip ultrasound?
The first encounter a child has with an orthopedic surgeon usually involves a hip ultrasound. Hip ultrasound and clinical examination of an infant (a child aged four weeks to one year) primarily serve to detect and treat the most common musculoskeletal diseases in infants, such as congenital hip dysplasia (developmental dysplasia of the hip), torticollis, and foot deformities. Although the majority of children are born healthy and without musculoskeletal issues, timely hip ultrasound and examination by a pediatric orthopedist are desirable as all difficulties can be treated more quickly, successfully, and easily with early therapy.
When to take a child for a hip ultrasound?
For children born at term, from the 39th week of pregnancy onwards, it is best to perform a hip ultrasound at five to eight weeks of age. However, for children with a family history of someone being treated with Pavlik harnesses as an infant, experiencing childhood limping, or similar situations, it is advisable to perform a hip ultrasound a bit earlier. Positive family history, breech position during pregnancy (regardless of whether the birth was vaginal or cesarean), and a lack of amniotic fluid during pregnancy (oligohydramnios) are risk factors for the development of congenital hip dysplasia. However, congenital hip dysplasia, or as it is commonly referred to, hip dislocation, is a genetic condition present in the fetus in the womb. Therefore, the statement “Hips dislocated during birth because he/she was breech” is not considered accurate.
How is a hip ultrasound done?
In Croatia, the Graf method of hip ultrasound is accepted, where the infant is placed in a lateral position, and the ultrasound probe is placed laterally on the upper part of the observed thigh. It should be noted that hip ultrasound is a subjective imaging method, and for a technically correct diagnosis and interpretation, knowledge and skills acquired through practice in a clinic are required.
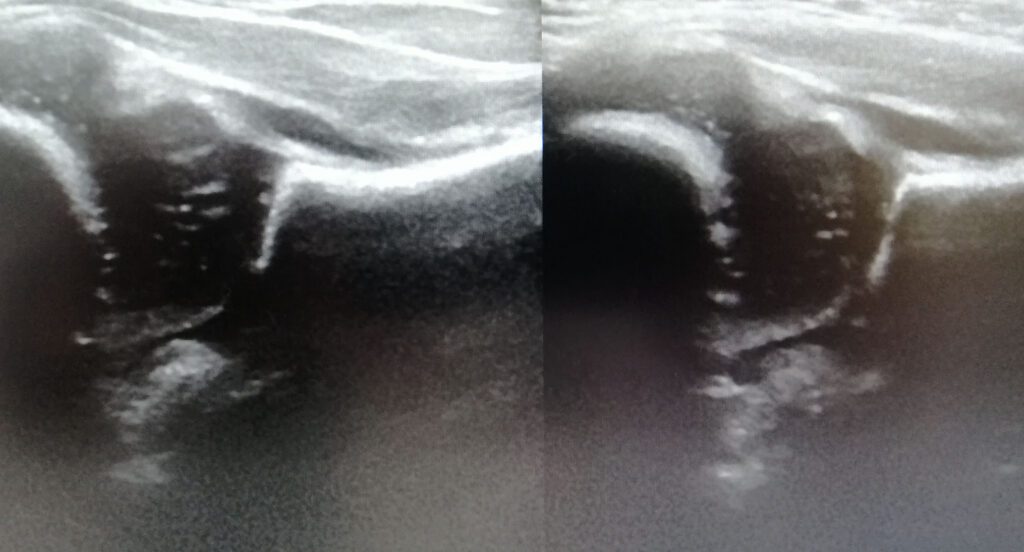
Figure 1.
What can be detected with hip ultrasound?
Hip ultrasound in infants is the so-called gold standard for detecting congenital hip dysplasia. Being dysplastic means being irregularly developed. In the case of congenital hip dysplasia, this means that the hip socket on the pelvis is too shallow, and the head of the femur does not sit properly in its place, causing the hip joint not to develop properly. Essentially, through hip ultrasound in infants, the aim is to see whether the hip is developing correctly or if it is too shallow. Image 1 shows a normal ultrasound appearance of infant hips. If hip dysplasia is detected through ultrasound, treatment should be initiated as soon as possible. Dysplasia may not be present on both hips, usually occurring on the left and more commonly in female children.
What if congenital hip dysplasia is detected?
Since congenital hip dysplasia has different clinical manifestations – degrees, treatment needs to be adapted to the severity of dysplasia and the child’s age. Discovered in time, dysplasia is mostly treated conservatively with Pavlik harnesses, and if the child is younger and less mature, attempts can be made with abduction braces. If hip dislocation accompanies dysplasia, the Hilgenreiner method or casting may sometimes be necessary. All these methods aim to position the femoral head above the dysplastic – shallow socket and, in that position, mechanically press the head to deepen the socket. This is possible while children are young, and the hip socket is cartilaginous and can be plastically reshaped. Unfortunately, sometimes congenital hip dysplasia is not detected in time, and the possibility of plastic reshaping is small, requiring immediate surgical interventions. The purpose of all treatments for congenital hip dysplasia is to establish a more correct relationship in the hip joint and later achieve optimal joint function—namely, pain-free and full range of motion. Untreated hip dysplasia leads to irregular wear of the hip joint cartilage, the emergence of pain, limping, and the development of secondary osteoarthritis, ultimately requiring treatment with the installation of a prosthesis – an artificial hip joint.

